…τα χριστουγεννιάτικα δώρα εννοεί η κούκλα!
Συνάδελφοι Συνεδέλφισσες
Νέα μέλη ΔΕΠ(Επίκουροι Καθηγητές) στη Ακαδημαϊκή Καρδιολογική Οικογένεια του EKΠΑ: Χριστίνα Χρυσοχόου, Κ. Αζναουρίδης, Αρώνης, Μ. Αντωνόπουλος, Π. Δηλαβέρης, Γ. Καραμάσης, Χ. Καπέλιος, Στ. Γεωργιόπουλος, Γ. Βλαχογιάννης, και ακολουθούν ακόμη 5 ! Είπαμε αν έχεις μπάρμπα(πρύτανη) στη Κορώνη!
Πολλές υποψηφιότητες και τέλεια βιογραφικά. Θερμά συγχαρητήρια και καλή σταδιοδρομία! Να θυμάστε ότι ο κύριος σκοπός σας (γι αυτό εξάλλου πληρωνόμαστε) είναι η εκπαίδευση των φοιτητών αλλά κρινόμαστε από την έρευνα(παραγωγή νέας γνώσης) …και από λίγο τσατσιλίκι(πχ να γελάτε δυνατά στα κρύα ανέκδοτα του Δτου σας) που ισχυρίζονται οι λίγοι κακεντρεχείς!
Και έξω καλά πάμε. Η Ιουλία Γράψα(απόφοιτος Ιατρικής Ιωαννίνων) έγινε αναπληρώτρια καθηγήτρια με εξειδίκευση στους υπερήχους και διευθύντρια Εκπαίδευσης(director for Education) στην Ιατρική του HARVARD.
Tον Κων/νο Λυκέτσο(υιός του αείμνηστου καθηγητή μας στη Ψυχιατρικής) κορυφαίο ερευνητή του Αλτσχάιμερ (John Hopkins VALTIMORE) βράβευσε η Ακαδημία Αθηνών.

JAMA Cardiol 2024;9:1159-1168. Aπό το 1968- Ross & Braunwald = είναι γνωστά τα συμπτώματα της σοβαρής στένωσης αορτής: στηθάγχη, συγκοπή(αιφνίδιος θάνατος) και δύσπνοια (καρδιακή ανεπάρκεια) και ότι η εμφάνιση τους έχει δυσμενή πρόγνωση.
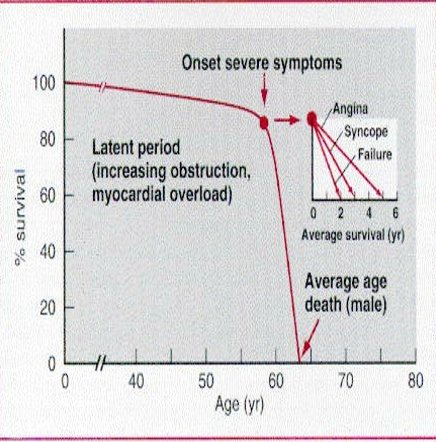
Σχεδόν 75% των συμπτωματικών ασθενών με σοβαρή στένωση αορτής θα πεθάνουν μεσα σε 3 χρόνια χωρίς αντικατάσταση,
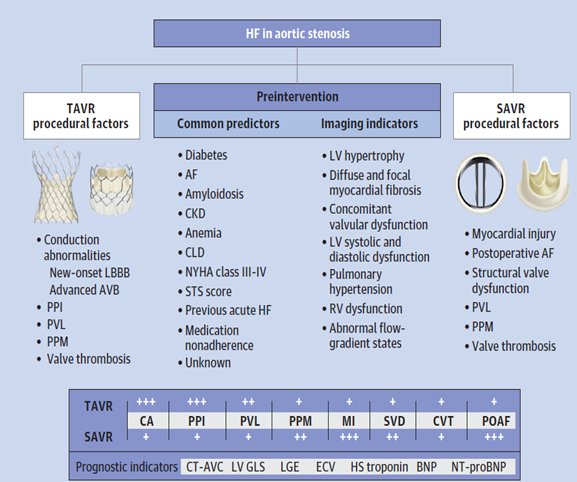
key points from a review on aortic stenosis (AS), heart failure (HF), and aortic valve replacement (AVR):
- AS is responsible for the development of HF that is mediated both by AS-associated chronic pressure afterload and subsequent unfavorable cardiac remodeling that includes LVH with impaired coronary microvascular function and eventual myocardial fibrosis.
- Evidence of LV impairment caused by AS can be detected using echo global longitudinal strain imaging for occult myocardial dysfunction, and MRI for evidence of focal myocardial fibrosis (using late gadolinium enhancement) or diffuse interstitial myocardial fibrosis (using T1 mapping and myocardial extracellular volume quantitation).
- Serum biomarkers including natriuretic peptides and troponin can serve as surrogate markers to help identify patients with asymptomatic or moderate AS who might benefit from earlier intervention.
- Both patient-related and procedure-related factors can contribute to HF among patients who undergo AVR for AS.
- Patient-related factors include diabetes, which worsens LV remodeling and affects both systolic and diastolic LVF; cardiac amyloidosis; AF; concomitant VHD including mitral regurgitation and/or tricuspid regurgitation; and concomitant CAD, which can exacerbate myocardial ischemia and therefore LV dysfunction.
Procedure-related factors include conduction disturbances and permanent pacemaker implantation(PPI) with resulting LBBB; abnormalities in valve performance including paravalvular leak(PVR) after transcatheter aortic valve replacement (TAVR) and moderate or severe prosthesis-patient mismatch, more common after surgical aortic valve replacement (SAVR); and myocardial injury after either SAVR or TAVR.
5.Mid-term data suggest that HF hospitalization is more common after SAVR than after TAVR, although long-term data still are outstanding.
6.Guidelines on the management of patients with valve disease do not include recommendations specific to the treatment of HF before or after AVR for AS. Published data suggest that treatment with RAS inhibitor therapy (but not β blockers) is associated with decreased all-cause mortality and HF hospitalization.
7.ΣΥΓΓΕΝΕΙΣ ΚΑΡΔΙΟΠΑΘΕΙΕΣ ΕΝΗΛΙΚΩΝ
Budts W, Prokšelj K, Lovrić D, Kačar P, Gatzoulis MA, Brida M. Adults With Congenital Heart Disease(CHD): What Every Cardiologist Should Know About Their Care. Eur Heart J 2024;45:4783-4796.
George G καμία Ελληνική βιβλιογραφική αναφορά!
Principle 1: Track medical and surgical history. An accurate understanding of the underlying anatomical diagnoses and previous procedures is key to understanding a patient’s current physiology and to guide appropriate testing and patient care.
Principle 2: Look for the expected. Know basic outcomes for the specific congenital heart defects. Each congenital heart lesion is associated with a number of long-term issues requiring monitoring and follow-up. A knowledge of these issues allows for a high index of suspicion for certain long-term complications, such as pulmonary valve regurgitation and ventricular tachyarrhythmias in patients with ToF. The authors provide a concise summary of common lesions and their associated issues.
Principle 3: Unravel the unexpected. Patients with complications not consistent with their underlying anatomy require additional evaluation to identify co-existing congenital or acquired issues. There should be a low threshold for expert adult CHD consultation in these situations.
Principle 4: Employ appropriate diagnostic tests and interpret accordingly. Echo, CT, MRI, and cardiac cath all play important roles in the evaluation of adults with CHD. Multiple congenital cardiac anomalies may co-exist in the same patients. Congenital expertise should be employed in the interpretation of noninvasive and invasive testing when necessary.
Principle 5: Deal appropriately and promptly with emergencies. arrhythmias, systemic right ventricular failure, endocarditis, and complications of right-to-left shunting.
Management of specific emergencies:
- Atrial arrhythmias should be suspected in any tachycardiac CHD patients. There should be a low threshold for prompt cardioversion to restore sinus rhythm.
- “Never trust a systemic or single right ventricle.” These patients are at risk for sudden decompensation, particularly in the setting of arrhythmias.
- Be aware of right-sided endocarditis, particularly in patients with bioprosthetic valves.
- Be aware of paradoxical embolism in systemic vasodilation in patients with obligate right-to-left shunts.
Principle 6: Provide advice regarding everyday life: education, work, sport, and pregnancy. Counseling regarding appropriate vocations, exercise prescription and restrictions if necessary, and pregnancy risks and management are key parts of the management of adults with CHD.
Principle 7: Seek expert adult CHD advice. Regular follow-up at specialized centers for more complex CHD is required. Even patients with simple lesions benefit from intermittent evaluation at experienced adult CHD centers. Direct communication between local and tertiary centers with a collaborative approach allows for optimal patient care.
Για κάτι απλό-πραχτικό για αυτό το μη συνηθισμένο θέμα ανατρέξτε στο www. Elikar.gr. Tσαγγαλίδου Ε, Βασιλειάδης ΚΕ, Γουδέβενος Ι. Συγγενείς καρδιοπάθειες που πρώτο διαγιγνώσκονται στην ενήλικο ζωή. Καρδιά ∞ Αγγεία 2018, 23:331-341
ΑΝΤΙΜΕΤΩΠΙΣΗ ΑΡΡΥΘΜΙΩΝ ΜΕΤΑ ΕΓΚΕΦΑΛΙΚΟ
Spooner MT, Messé SR, Chaturvedi S, et al. 2024 ACC Expert Consensus Decision Pathway on Practical Approaches for Arrhythmia Monitoring After Stroke: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol 2024;Dec 17:[Epub ahead of print].
- Stroke is a leading cause of death and disability worldwide. Atrial fibrillation (AF) is the most common arrhythmia that adults experience. AF increases the risk of stroke approximately five-fold. Detection of AF following stroke has significant implications on treatment decisions.
For patients with AF-related ischemic stroke, the primary treatment choice includes oral anticoagulation therapy. However, patients experiencing ischemic stroke without detectable AF are typically treated with antiplatelet therapy.
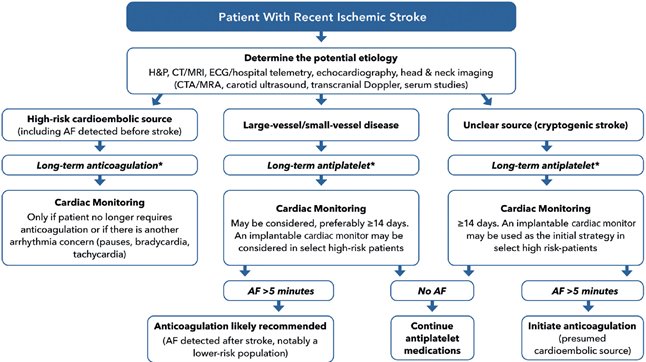
*All stroke patients require optimized medical management (high-intensity statin, long-term BP control, long-term glucose control, lifestyle interventions
Δεν αναφέρει το χρόνο έναρξης της αντιπηκτικής θεραπείας όταν η αιτία του ΑΕΕ είναι ΚΜ.
- Traditional methods of AF diagnosis, including ECG , often fall short in capturing transient AF. Longer duration of monitoring can increase the rate of AF detection. But the longer the time interval between the ischemic stroke and the detected AF episode decreases the likelihood of AF as a proximal cause of the prior event.
- Various technologies have been developed to identify AF, including continuous or intermittent ambulatory ECG monitors. There are also medical-grade monitors (typically electrical activity monitoring) and consumer-grade monitors (either electrical activity monitoring or photoplethysmography).
- Arrhythmia monitoring after a stroke requires three important steps. 1), a multidisciplinary evaluation should be undertaken to identify potential mechanism for stroke. 2], risk assessment is performed to determine the likelihood that a cardiac arrhythmia played a role in the stroke (or future stroke). 3, an optimal monitoring strategy should be selected to be accurate, practical, and establish follow-up.
- For patients with a high-risk cardioembolic source (including those with AF detected before the stroke), long-term anticoagulation is recommended. Cardiac monitoring is only needed if a patient no longer desires or requires anticoagulation therapy or if there is concern for another arrhythmia (e.g., bradycardia, pauses).
- For patients with large- or small-vessel disease, long-term antiplatelet therapy is recommended. Cardiac monitoring may be considered, preferably for ≥14 days. An implanted loop recorder can be considered in high-risk patients.
- For patients with an unclear source of their stroke (i.e., cryptogenic), long-term antiplatelet therapy is recommended. Cardiac monitoring is recommended for ≥14 days, especially if they are a candidate for anticoagulation therapy. An ILR may be used as the initial strategy in select high-risk patients.
- For patients in whom arrhythmia monitoring detects >5 minutes of AF, anticoagulation is likely recommended(esp CHA2DS2-VASc score is ≥3). For those with no AF, continuing antiplatelet therapy is recommended.
- In patients with stroke from a presumed cardioembolic origin, there is a limited role for rhythm monitoring given that anticoagulation is presumed necessary. Monitoring should only be considered if there is discussion around stopping anticoagulation or other treatments based on rhythm detection.
- Consumer devices have important limitations for AF detection, notably requiring direct skin contact for accurate reading. Those equipped with ECG capabilities are superior to those using photoplethysmography alone. Even when ECG technology is available, it requires active measurement by the wearer and is not “continuous” as with the medical-grade devices.
AF detected by consumer wearable devices (eg, smartwatches) should be confirmed with ECG correlation or through additional testing (eg, with an ECG patch monitor).ΧΡΟΝΙΑ ΦΛΕΒΙΚΗ ΑΝΕΠAΡΚΕΙΑ Μη χειρουργική αντιμετώπιση. Fukaya E, Kolluri R. Nonsurgical Management of Chronic Venous Insufficiency(CVI). N Engl J Med 2024;391:2350-2359.

CVI manifests as a spectrum of signs and symptoms, including varicose veins, leg swelling, skin changes, and leg ulcers. The condition is caused primarily by venous hypertension.
• Venous hypertension is a multifactorial disease, the cause of which can be structural (e.g., venous reflux or obstruction) or functional (e.g., dependent edema, weak calf muscle, or obesity) or both. Functional CVI is caused by obstruction of venous return, which can be due to elevated central pressures (such as from obesity, obstructive sleep apnea, or right heart failure), lymphatic dysfunction, or a decrease in the forward momentum of blood flow (such as from poor calf and foot pump function or dependent edema), all of which can lead to venous hypertension, even in the absence of structural venous damage
• The diagnosis is based on information obtained from the history and PE; further diagnostic imaging with duplex ultrasound examination is helpful for assessing for structural causes.
• Treatment is aimed at reducing the patient’s symptoms, which do not always correlate with the findings on physical or ultrasound .
• Endovenous procedures and surgeries can be effective treatment options for structural , but nonsurgical treatment measures are the mainstay for functional or combined (functional and structural) venous insufficiency.
• Nonsurgical management includes reducing central venous hypertension, compression therapy, leg elevation, and exercises involving calf and foot flexion and extension that provide a pump-function effect
- CVI comprises a constellation of symptoms and clinical manifestation, ranging from asymptomatic spider veins and varicose veins to leg ulcers. Varicose veins and CVI of the legs impact millions of people worldwide.
- Beyond cosmetic issues, CVI increases the risk of VTE and is associated with substantial limitations in daily functioning and quality of life.
- Risk factors for CVI include older age, female sex, obesity, pregnancy, prior deep vein thrombosis, and prolonged standing. There are also genetic markers that increase the risk of varicose veins.
- Contraction of the foot and calf muscles initiates cephalad flow of blood and opens one-way valves within the lower extremity veins. These valves prevent retrograde flow when closed, encouraging blood flow from the feet back towards the heart. Venous valve dysfunction causes venous reflux, backflow of blood, and venous hypertension.
- CVI is caused primarily by venous hypertension, which can result from structural or functional etiologies. Structurally, veins can reflux or be obstructed. Functionally, dependent edema, weak calf muscles, and obesity can contribute to venous hypertension.
- The diagnosis of CVI is based on information obtained from a history and PE. Imaging tests are not required to make a diagnosis, but can be helpful to detect structural causes. PE should be performed in the upright position to observe the effect of gravity and body weight.
- Common clinical examination findings in CVI include hyperpigmentation (hemosiderin staining), scarred tissue (atrophie blanche), dilated reticular veins at the ankles and feet (corona phlebectatica), skin texture changes (lipodermatosclerosis), erythema, and skin breakdown (ulcers). Swelling is also a common finding. When swelling is seen on the dorsum of the foot and of the toes (Stemmer’s sign), this typically indicates lymphatic dysfunction.
- Many medications are known to cause leg swelling. These include antiepileptics (e.g., gabapentin), antidepressants (e.g., escitalopram, paroxetine, venlafaxine), antipsychotics, antiparkinsonian (e.g., levodopa, carbidopa), antihypertensive (e.g., amlodipine, doxazosin, hydralazine), hormone therapies (e.g., estrogen, testosterone), glucocorticoids, NSAIDs, chemotherapy, thiazolidinediones, and PPIs.
- The clinical, etiologic, anatomical, pathophysiological (CEAP) classification is useful for disease classification, while the Venous Clinical Severity Score (VCSS) is useful for assessing and documenting disease severity.
- Treatment is focused on reducing a patient’s symptoms, which do not always correlate with findings on physical examination or imaging test.
- Endovenous procedures and surgeries are effective treatment options for structural venous insufficiency. However, nonsurgical treatments are the mainstay of therapy for both structural and functional CVI.
- Nonsurgical management includes reducing central venous hypertension, compression therapy, leg elevation, and exercises involving the calf and foot flexion/extension that provide a pump-function effect.
- Obesity is an independent risk factor for CVI disease progression. Obstructive sleep apnea, diastolic dysfunction, and right heart failure all increase central venous pressure and lead to peripheral venous hypertension.
- Diuretics should not be a first-line therapy for swelling and should only be used for volume overload.
- Graduated compression therapy can considerably improve CVI symptoms, but there is little evidence that they are curative or slow disease progression. A compression level above 30 mm Hg is recommended for ulcer healing. Lower levels of compression (e.g., 20-30 mm Hg) are often used when patient compliance is a concern.
Venous hypertension leading to CVI can be both structural and functional
in nature. Addressing both aspects of this pathologic process is essential to achieve clinical improvement. Whereas structural issues can be addressed with venous procedures, functional issues must be addressed nonsurgically. For patients with symptomatic varicose veins and axial reflux in the great or small saphenous veins, first-line treatment with venous intervention is recommended over long-term compression stockings (class IB recommendation [strong with moderate quality of evidence]. The current class 1A recommendation (strong with high quality of evidence49) for venous leg ulcer healing is compression therapy; however, the 2018 EVRA trial showed that early venous procedures improve venous leg-ulcer healing
XΡΟΝΙΑ ΠΟΛΛΑ & ΚΑΛΕΣ ΓΙΟΡΤΕΣ ΒΡΕΕΕΕ!
Γουδέβενος Γιάννης Γιάννινα

Ν. Λύτρας 1904 κάλαντα. Πινακοθήκη E. Αβέρωφ Μέτσοβο.
