Συνάδελφοι
Θα ξεκινήσω με γκρίνια. Στο τελευταίο Hell J Cardiol 2025;85:81–89 δημοσιεύτηκε εργασία από Sagris M et al. Young and older patients with acute myocardial infarction. Κοιτάζοντας τις παραπομπές- references με έκπληξη διεπίστωσα ότι δεν υπήρχε αναφορά στο State of the Art Review Causes, Angiographic Characteristics, and Management of Premature Myocardial Infarction απο L. Rallidis et al. J Am Coll Cardiol 2022;79:2431–2449. Συνάδελφοι λίγο αλληλεγγύη και οι reviewers λίγο περισσότερη προσοχή
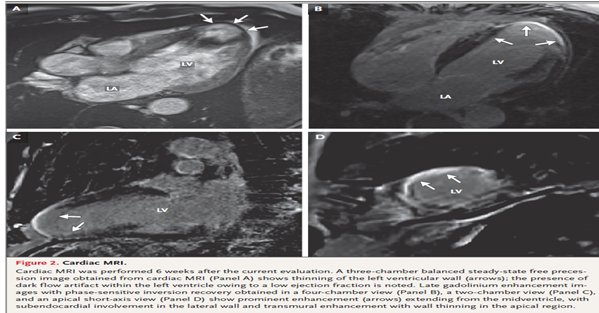
To Case 27-2025 από το Massachusetts General Hospital αφορούσε 53 χρονο με πολυεστιακά εμβολικά εγκεφαλικά(που συνηγορούν για καρδιακή και όχι αγγειακή προέλευση) από μη ισχαιμική μυοκαρδιοπάθεια(ΚΕ 28%) με ανεύρυσμα στη κορυφή και θρόμβο. Η διάγνωση ήταν ν. Chagas με αίτιο Trypanosoma cruzi. N Engl J Med 2025;393:1216-25. ESC 1225 In the PARACHUTE-HF study of patients with heart failure (HF) as result of Chagas disease, sacubitril/valsartan was superior to enalapril with respect to the primary endpoint of cardiovascular death, hospitalization for HF or the relative change from baseline to week 12 in NT-proBNP.
Αν ενδιαφέρεσθε για θρόμβο στη κορυφή μετά ΕΜ Christos Katsouras , X Sakellariou , A Bechlioulis, L Lakkas , P Korantzopoulos. Current insights and challenges in the management of left ventricular thrombus. Trends in Cardiovascular Medicine 2025 in press
Ο λαός συνήθιζε να λέει Οι άνδρες βγάζουν τα κουσούρια στο στρατό και οι γυναίκες στη γέννα.
Ειναί αλήθεια ότι σ στρατός αποτελούσε μεγάλο ηθμό για προβλήματα υγείας κυρίως με αλλεργίες.

Αναφυλακτικό shock και θάνατο από αντιβιοτικά έχω δεί με ενέσιμο amoxyl. H δράση είναι όσο πιο γρήγορα γίνεται παρεντερική χορήγηση αδρεναλίνης
Ο γιατρός που κατηγορείται για ιατρικό λάθος/αμέλεια Ζει τον πόνο εντελώς μόνος του. Κανείς φίλος ή συγγενής ακόμη και η/ο σύντροφός σου δεν μπορεί να καταλάβει το δράμα σου. …και τα βάσανα δεν έχουν τελειωμό
Θα χρειασθείς καλό δικηγόρο αλλά θέλει πολλά λεφτά

…και ν ακούς στα πρωινάδικα τη σωστή διάγνωση που εσύ έσφαλες. Και από κοντά οι μαϊντανοί Γιαννακός(… να δούμε αν ακολουθήθηκε το πρωτόκολλο είπε) και Ματίνα. ΕΛΕΟΣ!
BAΛΒΙΔΟΠΑΘΕΙΕΣ
Δεν μας αρκούσαν οι ESC 25 guidelines και ο Καταιγισμός πληροφοριών συνεχίζει !!!
ΣΤΕΝΩΣΗ ΑΟΡΤΙΚΗΣ ΒΑΛΒΊΔΑΣ
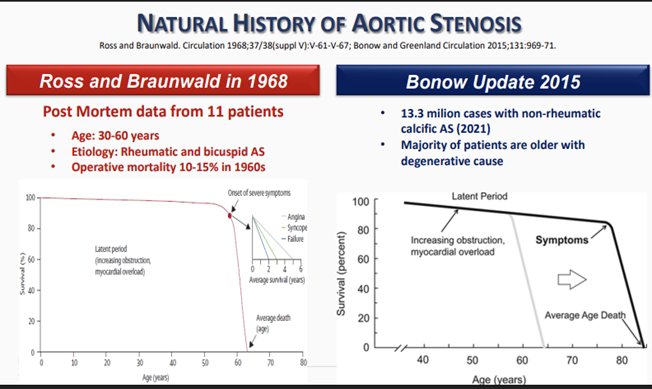
Γενεές γιατρών γαλουχήθηκαν με το watchful waiting παράδειγμα
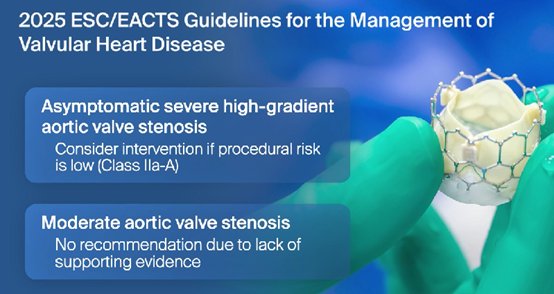
Η ασυμπτωματική στένωση αορτής Αποτέλεσε και αντικείμενο αντιπαράθεσης στο ESC 25
Η ασβεστωμένη αορτική βαλβιδική στένωση αποτελεί τη πιο συχνή μορφή αορτικής στένωσης Milind Y. Desai, Eugene Braunwald. The Pathophysiologic Basis and Management of Calcific Aortic Valve Stenosis JACC State-of-the-Art Review JACC. 2025;86:659–672)
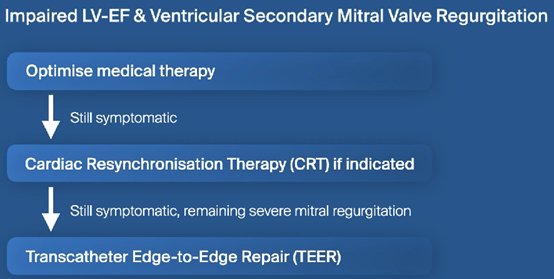
Ανεπάρκεια Μιτροειδούς Βαλβίδας(ΜR),
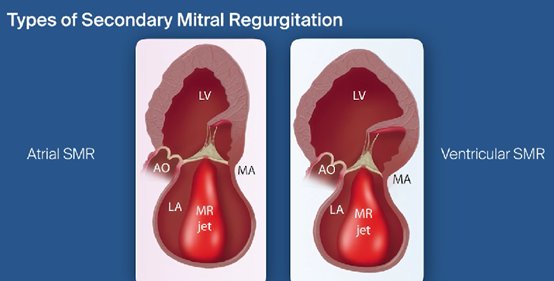
Secondary mitral regurgitation (SMR), also known as functional MR, is defined as MR secondary to LV or atrial disease in the absence of significant structural mitral leaflet abnormalities.
SMR can be further classified based on its pathophysiologic mechanisms and clinical presentations as well as on its severity. The first classification differentiates between ventricular SMR, typically associated with HFrEF and driven by LV dilation and papillary muscle displacement, and atrial SMR, more commonly observed in HFpEF, which results from isolated LA) dilation and mitral annular enlargement, often coexisting with AF.
Για τη πρωτογενή MR χειρουργείο και κατά προτίμηση επιδιόρθωση(repair)
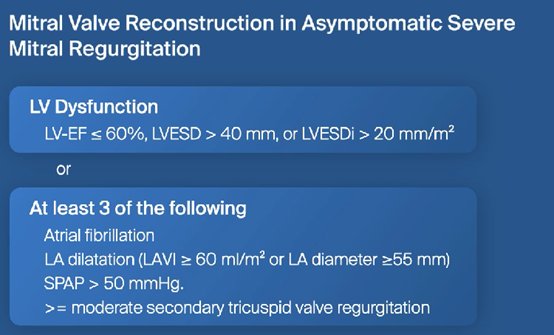
Για δευτερογενή MRΤΕΕR
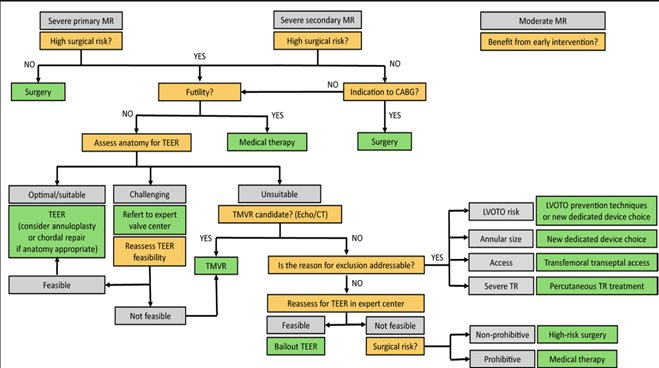
Ενας απλός αλγόριθμος για την αντιμετώπιση ης ανεπάρκεια της Μιτροειδούς(ΜR). Transcatheter MV replacement (TMVR) for the Treatment of Mitral Regurgitation: A State-of-the-Art Review: Circ Cardiovasc Interv. 2025;18:e015298
Future trials are needed to determine whether M-TEER should be routinely offered to HF patients with moderate
STATE-OF-THE-ART REVIEW: Moderate Secondary Mitral Regurgitation. JACC. 2025;86:813–828 2025 ACC Expert Consensus Decision Pathway. 10 Issues for the Clinician in Tricuspid Regurgitation(TR) Evaluation and Management. JACC 2025 on line
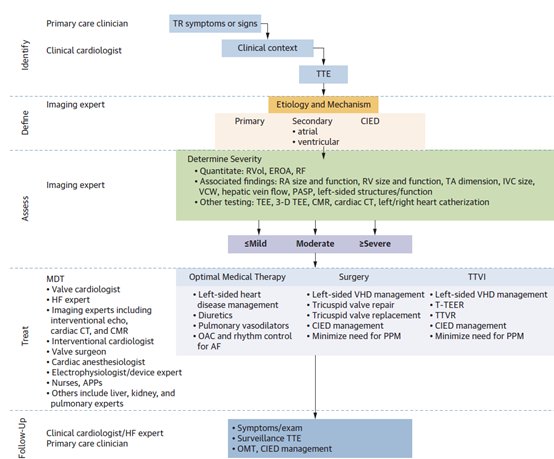
Focuses on the recognition, diagnosis, and assessment of TR, with imaging experts tasked with determining the etiology, mechanism, and severity. TTE is the key imaging modality for evaluation, although the document highlights the role of more advanced techniques, like CMR and cardiac CT, as well. Adjunctive features, like right heart size and function, that should be considered, as well as the natural history of TR, which can go undetected for some time before it’s clinically recognized. They include models for assessing 1- and 3-year risks of all-cause mortality.
The first message is it’s very important to have an accurate diagnosis of ΤR.
Treatment Options
There are no disease-modifying therapies with specific indications for treating TR, but the magnitude of TR can be eased by treating HF due to left-sided heart disease and AF.
There are sections on use of diuretics, GDMT) for underlying disease, and pulmonary vasodilators, as well as on therapeutic considerations for RV failure, AF, and TR related to CIEDs.
The document also covers the consequences of progressive TR and RV dysfunction, issues around cardiorenal and cardiohepatic syndromes, and referral to advanced HF teams.
There is much discussion of options for surgical and transcatheter treatment of TR, the latter including not only T-TEER and TTVR, but also annuloplasty and heterotopic caval valve implantation.
The authors point out that certain variables can be used to indicate that T-TEER or TTVR may be preferred over the other. Having septal-lateral coaptation gaps > 7 mm or more than three TV leaflets or scallops, for instance, may favor TTVR,
whereas the presence of advanced renal function or an inability to take anticoagulation may favor T-TEER.
Most patients actually end up not needing a procedure. They’re either medically managed or a lot of times they’re sort of so far advanced that they probably need palliative care inputs.
There is a role for the transcatheter therapies for patients in between those two types of populations. I don’t envision that this would be used indiscriminately, because TR is very prevalent. It just depends on really having a great understanding of the mechanism and where the patient is on that spectrum with the TR.
O’Gara PT, Lindenfeld J, Hahn RT, et al. 10 issues for the clinician in tricuspid regurgitation evaluation and management: 2025 ACC expert consensus decision pathway. JACC 2025;Epub ahead of print.Ότι προσδοκάτε για ΚΑΡΔΙΑΚΗ ΑΝΕΠΆΡΚΕΙΑ. To εγγυάται η ιέρεια της ΚΑ Χριστίνα Χρυσοχόου. Η μοναδική(only and one) Ελληνίδα καρδιολόγος στο World’s Top 2% scientist list.(Stanford, Ioannidis 2024)

Συναδελφικά
Γουδέβενος Γιάννης Γιάννινα
