
ή …κούρευε λαγούς και άρμεγε χελώνες.
Συνάδελφοι Συναδέλφισσες
ΑROUND THE WORLD ACROSS GREECE
Mόνο στη Ελλάδα συμβαίνουν. Η ομάδα εργασίας Ηλεκτροφυσιολογίας της ΕΚΕ στις 27 3 διοργανώνει webinar για την υποκλινική ΚΜ και τη χρήση DOACs με τις δύο κλασσικές μελέτες NOAH – AFNET 6 και ARTESiA.
Στην πρώτη μελέτη έχει πάρει μέρος η καρδιολογική κλινική του Ηρακλείου και στη συγγραφική ομάδα συμμετέχουν και Ελληνες συνάδελφοι(όχι κάτι σύνηθες). Θα περίμενες να τους δεις στο webinar αλλά απουσιάζουν. Το επισημαίνω με επιφύλαξη παρ ότι γνωρίζω ότι ο νυν πρόεδρος της ομάδας τα προσέχει αυτά.
Tην παγκόσμια ημέρα της γυναίκας η Επιτροπή Γυναικών Ιατρών του Πανελλήνιου Ιατρικού Συλλόγου έκανε εκδήλωση με τίτλο «Γυναίκες Ζωής, Γυναίκες Αξίας, Γυναίκες Ιστορίας» και τίμησε 8 γυναίκες γιατρούς. Ούτε μια καρδιολόγος!
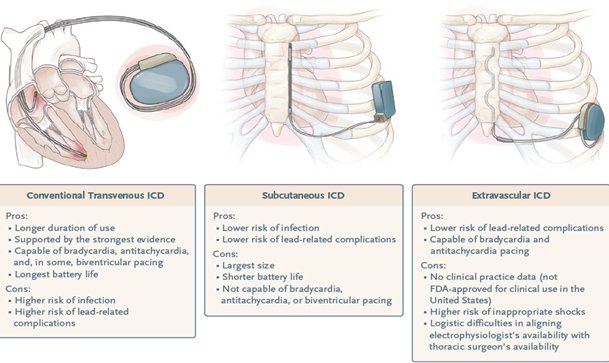
Υπέρ και κατά(prons and cons) των διαφόρων ειδών ICD. N Engl J Med 2024;390:442-54.
Στη καρδιολογική του Ευαγγελισμού από το Σωτ Ξυδώνα τοποθετήθηκε ο πρώτος στην Ελλάδα extravascular ICD. Eπανειλημμένα έχουμε μνημονεύσει την εκπαιδευτική δραστηριότητα της ESC που αξίζει να παρακολουθήσετε.

https://esc365.escardio.org/esc-tv-today . Διαρκεί 20 min και είναι κάθε 2ρη Πέμπτη. Next 28 Μαρτίου.
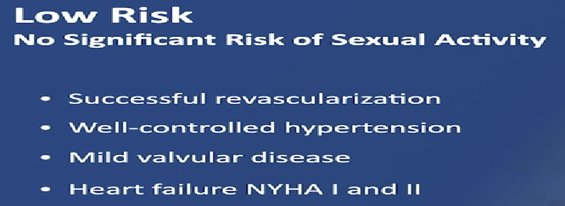
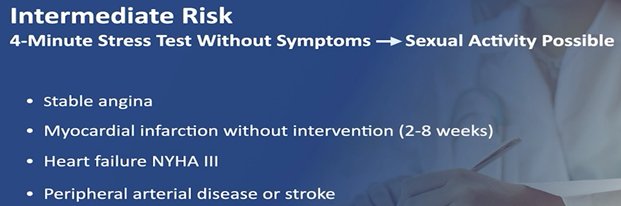
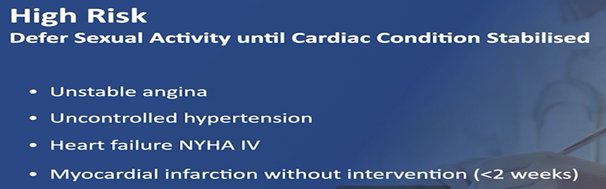
Το πρόσφατο esc tv today είχε θέμα: σεξουαλική δραστηριότητα και ΚΑ παθήσεις. Γενικά πρόκειται για χαμηλού κινδύνου αλλά ο κίνδυνος υπαρκτός. Στη φάση του οργασμού η ΚΣ φτάνει τις 130 σφύξεις/λεπτό και ΣΑΠ 170 mmHg και διακρίνονται σε 3 κατηγορίες κινδύνου με συχνότερη και τη πιο προβληματική για προσέγγιση την ενδιάμεση.
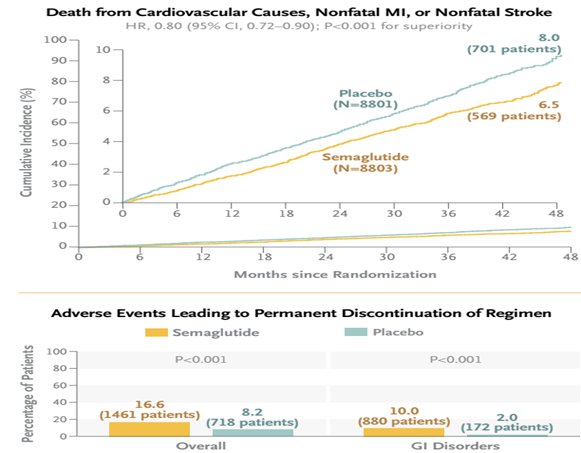
H σεμαγλουτίδη(Ozempic) 2.4 mg SC απαξ εβδομαδιαία για παχύσαρκους/ υπέρβαρους με γνωστή ΚΑ πάθηση(δευτερογενή πρόληψη) έγινε αποδεκτή από το FDA βάσει της μελέτης SELECT. N Engl J Med 2023; 389:2221-2232

Περιστατικό της Εβδομάδας: Μυοκαρδιακή Γέφυρα
Aνδρας 66 χρονών με παράγοντες κινδύνου(υπέρταση, διαβήτης, ισχαιμικό ΑΕΕ) παραπέμπεται σε τριτοβάθμιο κέντρο μετά από καρδιακή ανακοπή. Για 6 μήνες ανέφερε πόνο στο στήθος και την ημέρα τη ανακοπής ξύπνησε με πόνο στο στήθος, έχασε τις αισθήσεις του και επανήλθε με ΚΑΡΠΑ από την οικογένεια. Στο νοσοκομείο είχε καλό υπέρηχο(;HKΓ) και η ΣΦ έδειξε 50% στένωση στον LAD στην διαστολή και πλήρη απόφραξη στη συστολή(Α). Εγινε διάγνωση μυοκαρδιακής γέφυρας(ΜΓ) (bridging). H ΜΓ είναι μια ανωμαλία των στεφανιαίων που μια επικάρδια στεφ αρτηρία πορεύεται ενδομυοκαρδιακά. Συνήθως είναι ασυμπτωματική και αργά στη ζωή ίσως παρουσιάσει λόγω συνυπάρχουσας υπερτροφίας ή μικρο αγγειακής νόσου ή αθηροσκλήρωσης. Eπειδή αποφασίσθηκε χειρουργική επαναγγείωση έγινε CTA που έδειξε 8 mm βάθος του mid LAD (C).Υπεβλήθη σε CABG με φλεβικό μόσχευμα και είναι ελεύθερος συμπτωμάτων.
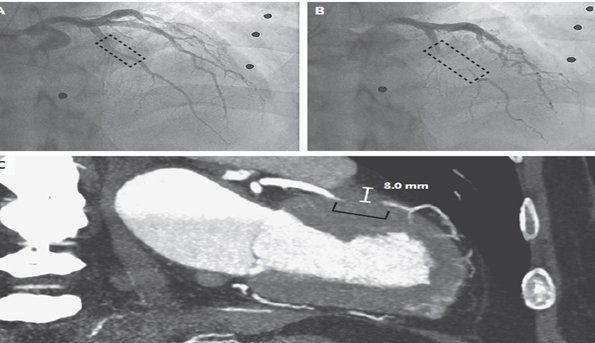
Περισσότερα στο Αφροδίτη Τσιάκου, Δ. Νίκας, Ι Γουδέβενος. Καρδιά & Αγγεία 2015;Iούλιος-Αύγουστος;296-7
Η επέμβαση στο σημείο πρόσφυσης του μοσχεύματος είναι πολύ αιματηρή(προσωπική επικοινωνία με Στρ. Παττακό)
Το Stress Perfusion MRI επειδή γίνεται κυρίως με αγγειοδιασταλτικούς παράγοντες δεν αναδεικνύει μυοκαρδιακές γέφυρες! Ίσως είναι η μόνη περίπτωση που η συγκεκριμένη δοκιμασία δεν έχει θέση ή πρέπει να γίνει με δοβουταμίνη!
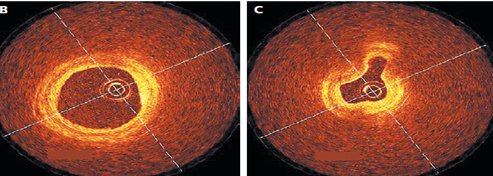
OCT στη διαστολή(Β) και συστολή (Α) σε μυοκαρδιακή γέφυρα στον mid LAD χωρίς στοιχεία αθηροσκλήρωσης
Συνέχεια αγνώστων λέξεων: palliative care(παρηγορική ή ανακουφιστική φροντίδα) συνήθως για τελικού σταδίου καρδιακή ανεπάρκεια(ΚΑ). Στις ΗΠΑ μόνο το 6% των ασθενών με σοβαρή ΚΑ τυγχάνει palliative care.
key points from a state-of-the-art review on palliative care across the spectrum of heart failure (HF):
- Patients with HF may be affected by a high symptom burden, poor functional status and quality of life (QoL), frequent hospitalizations, and high mortality rates. In addition, uncertainty about prognosis and potential treatment options, psychosocial and spiritual distress, and caregiver burden may impact overall care. Palliative care may help with addressing many of these issues.
- All clinicians caring for patients with HF should be able to address foundational palliative care needs (basic symptom management, identifying surrogate decision makers, discussing goals of care and preferences, helping with advanced directives), also referred to as primary palliative care. Specialty palliative care by those with specific training may provide additional benefit when symptoms become intractable or if complex medical decision-making and care for advanced disease management is required.
- In the ambulatory setting, specialty palliative care clinicians can help collaborate with the care team to manage symptoms, provide support and education to patients and caregivers, assist with advance care planning, and coordinate additional resources.
- In the hospitalized setting, which often represents a key clinical worsening in a patient’s overall trajectory, focus should remain on improving QoL, providing optimal HF GDMTs, assessing goals of care, and planning for effective transitions of care. In situations where HF treatment options are limited and prognosis is poor, the general focus of care is the same, though de-prescribing medications that do not provide symptom relief and using palliative inotropes can be considered.
- In patients with advanced HF, specialty palliative care may help patients to understand the potential benefits/risks/burdens with specific therapies (heart transplantation, LVAD) and the psychosocial impact (lifestyle changes, caregiver support, etc.). For patients who are ineligible for life-prolonging advanced therapy options, specialty palliative care can help patients and families adjust to new plans of care and potentially engage with hospice services.
- Home-based palliative and hospice care is an alternative to hospital-based programs for appropriate patients living with HF. Models for home-based care are still being developed, though they have the potential to serve the needs of many patients.
- Appropriate consideration needs to be given to caregivers and families, as they are key members of the care team and assume significant responsibilities (direct patient care, transportation, psychosocial support, etc.). Palliative care can assist with engaging caregivers and families in the decision-making and planning process.
- The evidence base for palliative care for patients with HF generally shows positive associations with outcomes. However, the studies are limited by small sample sizes, variable quality, and heterogeneous interventions and outcome measures. Future opportunities to enhance the palliative care evidence base include standardizing what a palliative care intervention should include and what outcomes are most appropriate and clinically relevant.
- The future vision of palliative care in HF includes being able to equitably provide access to care and to provide this care at the right level at the right time. Considering the shortage of trained specialty palliative care clinicians, new models of care and initiatives are needed. This may include providing more basic palliative care training to care team members (community health workers, primary care physicians, general cardiologist, etc.) and utilizing virtual care visits.
- To reduce disparities in palliative care utilization and referrals, it is recommended that systems be put in place to identify patients early in the disease course who may have unmet needs and to engage with community health workers to build trust in communities and remove barriers to care.
Palliative Care Across the Spectrum of Heart Failure. JACC Heart Fail 2024;Mar 6:[Epub ahead of print]
Performance and Quality measures
key points from a 2024 report of the ACC/AHA on performance and quality measures for adults with valvular and structural heart disease:
- The AHA/ACC Joint Committee on Performance Measures writing committee developed new measures to evaluate the care of patients with valvular heart disease in accordance with the “2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease,” which includes a comprehensive list of 11 measures (five performance measures and six quality measures) that can be clinically used in patients with valvular heart disease.
- The five performance measures fulfill the attributes of performance measures (e.g., high impact, targeting meaningful gaps in care, actionable, relatively low abstraction burden [in terms of cost, effort, and time], unlikely to have unintended consequences with their implementation), and are based on Class 1 clinical practice guideline recommendations and are the following:
- In patients with a mechanical valve prosthesis, there is high-level evidence that therapy with an oral VKA at an appropriate INR goal reduces the incidence of valve thrombosis, thromboembolic events, and associated morbidity.
- Patients with severe symptomatic AS have a high risk of death if aortic valve intervention is not performed, as high as 50% at 1 year. Both SAVR and TAVI are effective across the spectrum of surgical risk, with significant improvements in morbidity, death, and functional status.
- Patients with chronic severe AR) who either have LV dysfunction (EF] <55%) or who develop symptoms, have a high risk of death, LV decompensation, and deterioration of functional status if aortic valve replacement is not performed.
- Serial echo are essential to evaluate changes in LV function and structure in patients with asymptomatic chronic severe primary MR to guide management decisions.
- Patients with chronic severe primary MR who develop symptoms or LVEF <60% have a high risk of death, LV decompensation, and deterioration of functional status if mitral valve intervention is not performed.
- In addition, the five performance measures listed are appropriate for public reporting or pay-for-performance programs.
- The quality measures on the other hand are not ready for public reporting or pay for performance but may be useful for clinicians and health care organizations for internal review and quality improvement. Quality measures may be upgraded in the future to a performance measure status after being assessed in real-world clinical practice, or can be completely retired in certain instances. For example, instances in which performance measures could be retired include very high levels of performance (“topping out”) or new evidence showing marginal clinical impact or unforeseen adverse consequences, such as risk aversion. The quality measures are:
- Documentation of Risk and Heart Team Discussion Before SAVR or TAVI.
- AVR for Asymptomatic AS With LV Systolic Dysfunction.
- TAVI for Severe Symptomatic AS >80 Years of Age.
- Post-AVR Echo.
- Adequate Blood Pressure Control in AR Patients.
- Treatment for Symptomatic Severe Rheumatic Mitral Stenosis.
- All measures pertain to the outpatient setting except one quality measure that applies predominantly to the inpatient setting, which is documentation of risk and heart team discussion before SAVR or TAVI.
- The measures are well defined and include definite exclusions (e.g., hospice, palliative care, comfort care) and relative exceptions, which may be medical- or patient-related (e.g., active bleeding, patient refusal).
- Of the performance measures, four are related to proven therapies (one is a medical treatment and three are surgical or catheter-based interventions), and one pertains to a diagnostic modality.
- The one performance measure pertinent(σχετικό) to medical treatment pertains(αναφέρεται) to the prescription of a VKA (e.g., warfarin) in patients with mechanical prosthetic valves, which has been proven to prevent valve thrombosis and thromboembolic events.
- Three performance measures pertain to the implementation of an appropriate valve intervention in patients with the following: 1) severe symptomatic ΑS 2) chronic severe ΑR and 3) chronic severe primary MR.
- A notable quality measure is the objective documentation of risk while using a procedural risk score and documentation of a multifaceted heart valve team discussion whenever a valvular procedure or surgical intervention is being considered.
2024 ACC/AHA Clinical Performance and Quality Measures for Adults With Valvular and Structural Heart Disease: A Report of the AHA/ACC Joint Committee on Performance Measures. J Am Coll Cardiol 2024;Mar 14:[Epub ahead of print]
Καλή Σαρακοστή! Και ο ταραμάς με μέτρο! Eξ άλλου η γίδα δεν μασάει!
Γιάννης Γουδέβενος Γιάννινα
